
|
Getting your Trinity Audio player ready...
|
Last updated on August 9th, 2023
Here’s an important board exam fact: you can study, study, and still further study the DSM-5 and still incorrectly answer diagnostically-focused psychiatry board exam questions. How can this be? If you have ever felt that your exam performance is not as good as your knowledge base suggests it should be, the following insight will partly explain this discrepancy.
The discrepancy between knowledge and performance arises from a discrepancy between what you spend your time studying (and memorizing) and what the exam is testing you on. Specifically, many exam candidates focus on learning each psychiatric disorder’s diagnostic criteria. Well, you might think, “What else is there if not the diagnostic criteria?” In fact, the board exam is not so much testing you on each disorder’s criteria as it is on distinguishing one disorder from another. For example, you will NOT see a multiple-choice question like this: “Which of the following is a criterion of illness anxiety disorder?” Rather what you will see is a short case vignette followed by the question: “Which disorder is this patient most likely to suffer from?” (Or some similarly worded version of this.)
Notice that the most common way of studying the DSM-5 is to read through and try to memorize the diagnostic criteria. But what you are tested on suggests that you should ALSO spend time studying the distinguishing features among a set of related disorders. To stress: only a small number of criteria are the distinguishing ones. I provide you two sets of examples (somatic symptom disorders and eating disorders) and a couple of sample questions.
Somatic Symptom Disorders
Somatic symptom disorders have been heavily revised – through simplification – in the DSM-5. The three specified disorders are: somatic symptom disorder, conversion disorder, and illness anxiety disorder. The somatic symptom disorders chapter also includes, as do all others, the category of “Other” disorders, Specified and Unspecified. I will ignore these “Other” disorders in this presentation. The criteria that distinguish the three main somatic symptom disorders can be shown in a table.
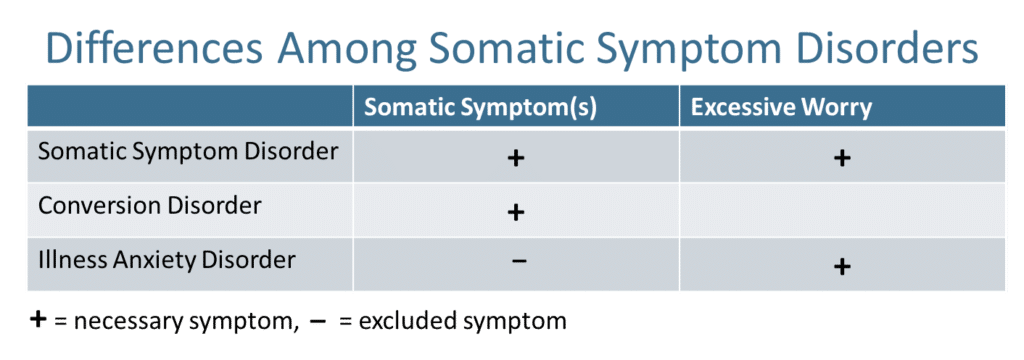
Take a look at your DSM-5. It’s astounding how simple the differentiation among the disorders can be. Of course, there are additional diagnostic details to keep in mind, but these details should only be added to and contained within the simple differentiating structure presented in the table above. For example, the somatic symptoms in somatic symptom disorder and conversion disorder differ: conversion disorder is characterized by a specific type of somatic symptom (loss of sensory or motor function) and this symptom remains medically unexplained. In somatic symptom disorder, the somatic symptoms are often not loss of sensory or motor function and they do not have to be medically unexplained. (Technically, however, the somatic symptom disorder criteria do NOT exclude medically unexplained loss of function symptoms.) Here is the wording from somatic symptom disorder’s differential diagnostic explanation of differentiating it from conversion disorder: “In conversion disorder, the presenting symptom is loss of function (e.g., of a limb), whereas in somatic symptom disorder, the focus is on the distress that particular symptoms cause. The features listed in criterion B of somatic symptom disorder [that is, the excessive worry symptoms] may be helpful in differentiating the two disorders.” Below are two vignette questions, the first describing somatic symptom disorder and the second illness anxiety disorder. And last point: illness anxiety disorder excludes presence of somatic symptoms unless they are slight.
Somatic Symptom Disorder Sample Board Exam Question
Question: 38 year old woman presents to the emergency department with chief complaint of “My awful pain is worse again.” She has had 43 previous emergency department visits for similar pain complaints in her “shoulders, back, pelvis and thighs.” She has been hospitalized twice for “suicidal ideation” and has a diagnosis of major depression and dependent personality disorder. She endorses a mutually abusive relationship with her spouse with whom she often drinks alcohol together “as our way of socializing.” Her previous work-ups for pain have yielded a diagnosis of “musculoskeletal pain” and she has been referred to physical therapy. What is her most likely diagnosis?
A. Body dysmorphic disorder
B. Conversion disorder
C. Adjustment disorder
D. Illness anxiety disorder
E. Somatic symptom disorder
Illness Anxiety Disorder Sample Board Exam Question
Question: 33 year old man presents to outpatient psychiatry with chief complaint of, “I believe I have stomach cancer but my doctor says ‘it’s all in my head’ because the gastroscopy was negative. But that scope can’t see through my stomach wall, just the inside surface.” Patient denies any change in eating and appetite, and identifies no problems with digestion, elimination, or pain. He says he’s stressed at work but says, “Isn’t everybody these days?” He says he started worrying about stomach cancer after vacationing in Thailand last year and eating “a lot of super spicy food.” He says he’s convinced that “could be the reason” for developing this disease. Medical records disclose normal physical exam and lab results after extensive work-ups. What is his most likely diagnosis?
A. Body dysmorphic disorder
B. Conversion disorder
C. Somatization disorder
D. Illness anxiety disorder
E. Somatic symptom disorder
Eating Disorders
Now let’s organize the symptoms in a table for the three specified eating disorders: anorexia nervosa, bulimia nervosa, and binge-eating disorder.
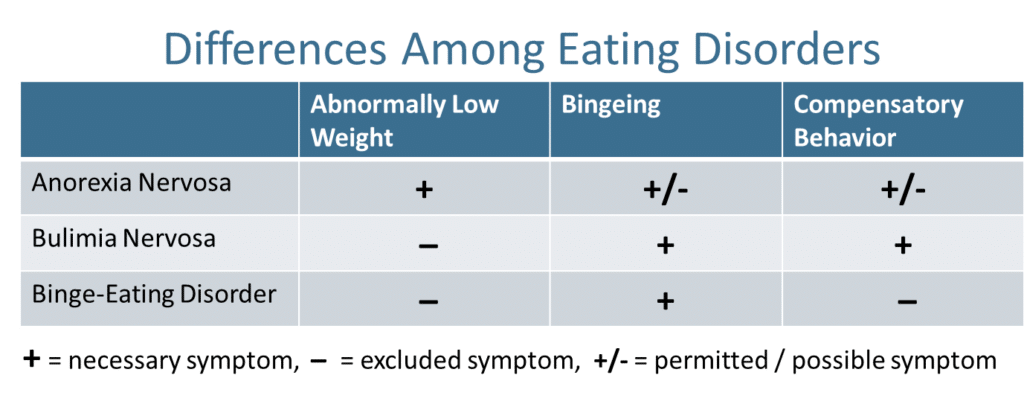
In eating disorders, anorexia nervosa is the only disorder associated with abnormally low weight, that is, any BMI < 18.5 kg/m2. Thus, any patient with abnormally low weight, even when bingeing and purging are present, is NOT diagnosed with bulimia nervosa or binge-eating disorder. Further, binge-eating disorder is differentiated from anorexia and bulimia by excluding presence of any compensatory behaviors. Compensatory behaviors include restricting and purging behaviors and either type of these compensatory behaviors can be present in anorexia and in bulimia. (Restricting behaviors include dieting, fasting, and excessive exercise.) Anorexia has two subtypes: one includes restricting behaviors only and the other includes either bingeing or purging behaviors.
Review these tables and work through these differences in your mind. Make up your own case vignettes or recall certain patients who met criteria for one disorder in a set and not others.
All the best on your exam.
![]()
Jack Krasuski, MD
If you need help preparing to take your boards you can access our board review courses for psychiatry and neurology at Beat the Boards, and all other medical specialities at The Pass Machine.

Excellent tables boils it down into a format that’s easy to recall. Thank you!
Glad you found the tables helpful in your review for the Psychiatry Board Exam. Thanks for reading! If you have anymore questions or thoughts do not hesitate to reach out to me.